

Thomas Beaney is a GP registrar and academic clinical fellow in primary care at Imperial College interested in the interface between primary care, public health and health policy. He is on Twitter: @DrThomasBeaney
Jonny Clarke is a Sir Henry Wellcome Postdoctoral Fellow and former surgical trainee at Imperial College, whose work focusses on understanding the complex dynamics between patients and organisations within the healthcare system. He is on Twitter: @Jonny_M_Clarke
For GPs to engage effectively and proactively in population health we need to understand not only who the population is, but also where they live. In this blog, we discuss our recent work exploring how upscaling GPs into Primary Care Networks (PCNs) can facilitate the provision of local place-based population healthcare.
General practice is well-positioned to identify and intervene in the wider determinants of health.
With the formation of PCNs in 2019 operating on broader geographical footprints, there is an expectation they will become key players in population health° management and in anchoring community providers.° The collaborations enabled by their formation have already shown benefits during the COVID-19 response,° with PCNs adapting dynamically to the local needs of their communities with respect to prescribing, testing and shielding of vulnerable patients.
In our recent article in BMJ Open° we used network-based clustering methods to identify how PCNs would best maximise the representation of their populations and understand their geographies, in order to better support the provision of population healthcare through primary care.
We found extensive overlap of the boundaries in which the population registered at each GP lives. This was particularly the case in urban areas with a high density of practices, and a relatively mobile patient population. Our study found that on average in London, within each small geographical unit, (Lower Layer Super Output Area, consisting of around 1,500 people) an average of five different GP practices provide primary care, with 5% receiving care from ten or more practices, which may hamper the ability of primary care to contribute meaningfully and efficiently to population health.
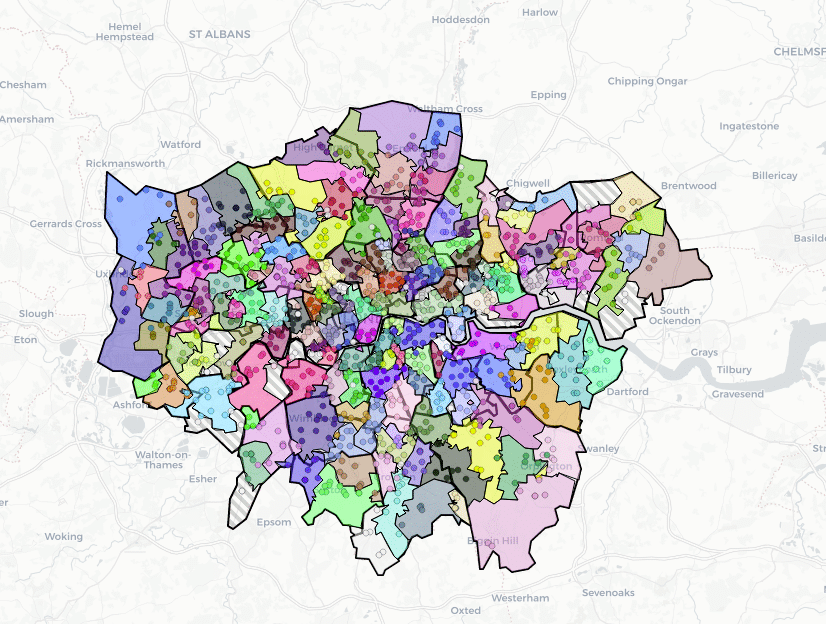
We found that by grouping GPs into larger communities in the form of PCNs using a purely data-driven approach, the local population coverage was much improved compared to that achieved by individual practices alone. Within the geography assigned to each PCN, on average 70% of the population were registered to a practice within the PCN, albeit with a wide range from only 45% in some areas to 91% in others. The interactive map displays how these PCNs in London emerged, along with the assigned geographies, which are exclusive to each.
The case for GP involvement in the health of their local communities has never been stronger
PCNs are still in the process of defining their roles and responsibilities, but over the course of a few months, many have been thrust into the centre of the primary care response to the COVID-19 pandemic. For their role in population health to be fully realised, an understanding is needed of both ‘who’ this population refers to, and ‘where’ this population resides, and our tool may aid in this purpose. Place-based delivery of care is under threat, but the case for GP involvement in the health of their local communities has never been stronger and we must preserve the community orientation of primary care.
Featured photo by Denise Chan on Unsplash





[…] CREDIT: This is an edited version of an articel that originally apepared on BJGP […]
[…] CREDIT: This is an edited version of an article that originally appeared on BJGP […]