

 Hugh Bethell is a retired GP and enthusiastic proponent of exercise as prevention and treatment of the non-communicable diseases of later life. He is author of Get Off the Couch Before It’s Too Late. More of Hugh’s work can be found at: https://cardiac-rehab.co.uk/blog
Hugh Bethell is a retired GP and enthusiastic proponent of exercise as prevention and treatment of the non-communicable diseases of later life. He is author of Get Off the Couch Before It’s Too Late. More of Hugh’s work can be found at: https://cardiac-rehab.co.uk/blog
During the COVID-19 pandemic, ‘Granny’ was identified as the archetypal older person who was very likely to die if she caught COVID-19. The presumption was that Granny was not only old but also frail, dependent, and probably in a care home. All of these factors certainly made her vulnerable. The accepted solution was to keep her isolated in the care home, lonely and unvisited by family or friends for fear they might infect her with the deadly virus — until she either got infected anyway or died from something else.
Both then and now there is no mention of prevention or treatment of Granny’s frailty. But frailty is not inevitable. The best thing we can do is to prevent Granny (and I include Grandad, so nearly all of us in the long term) getting frail in the first place.
What is frailty?
“… frailty is not inevitable. The best thing we can do is to prevent Granny getting frail in the first place.”
Frailty is officially described as ‘a clinically recognizable state of increased vulnerability, resulting from aging-associated decline in reserve and function across multiple physiologic systems such that the ability to cope with everyday or acute stressors is compromised’!1 In brief, old and feeble or weak and debilitated. Some of the essential features include low grip strength, low energy, slowed walking speed, low physical activity, and/or unintentional weight loss.2
Frailty is closely allied to loss of muscle tissue. As we age we all lose muscle mass and strength, a condition called sarcopenia. The prevalence of sarcopenia increases with each 5-year age group from about 15% for those aged 65–70 years to as much as 50% in those aged over 85, and probably becoming increasingly common thereafter. As the age of the population grows so will the numbers with sarcopenia.3
The ability of Grannies to function independently depends largely on them maintaining sufficient physical fitness and muscle strength to perform the activities of daily living.4 Tasks perceived as requiring substantial effort in deconditioned individuals tend to be avoided, setting off a vicious circle of further reduction in physical fitness causing further avoidance of physical activity and further loss of muscle mass and strength — and so on …
The effect of frailty is seen most obviously in the ability of older people to undertake daily tasks, such as getting up and dressed without help. Just looking after herself demands that Granny has a degree of physical fitness.5 If she can’t do these things she will become dependent on others to help. She will then need regular visits from carers or, worse still, admission to a care home.
A degree of age-related sarcopenia is unavoidable but the rate at which we lose muscle is largely dependent on how much exercise we take. This is what frailty is all about — and it is not an inevitable consequence of ageing but, at least in part, a lifestyle choice.
“… age-related sarcopenia is unavoidable but the rate at which we lose muscle is largely dependent on how much exercise we take.”
How has Granny got like this?
Frailty is associated with loss of muscle strength and low cardiorespiratory fitness. It is caused by taking very little exercise over a very long period.6 The resulting weakness is greatly aggravated by developing one or more of the degenerative diseases of later life such as heart disease, diabetes, lung disease, osteoporosis, and/or loss of balance — together called non-communicable diseases (NCDs). They are all promoted by lack of exercise further decreasing physical fitness and leading to the downhill spiral into frailty. For many older people, hospital admission is the final straw. Weakness makes Granny unsteady on her feet and at risk of falling. If she falls and is admitted she is in trouble. A week in hospital has been equated to an extra 5 years of loss of strength and mobility.7
Frailty is not inevitable
We all know people who are active and energetic into their late 80s and 90s. As a GP, I had many patients who told me how lucky they were to be so well in old age. My response was always the same — that they were not lucky but had looked after themselves, mainly by keeping very active.
An example of this effect was seen in a study of cycling club members aged 55–79 years. This group had high levels of fitness. For those aged 55 the fitness was equivalent to the average for those aged 20 years; for those aged 65 years it was equivalent to the average for those aged 25 years; and for those aged 75 years it was equivalent to the average of those aged 35 years!8
The improved health status of older people who have exercised regularly has been well illustrated by one study, which showed that achieving >150 min/week moderate-intensity aerobic exercise, such as walking or other moderate-intensity aerobics-type activities, is associated with at least 30% lower risk of morbidity, mortality, and functional dependence compared with being inactive.9
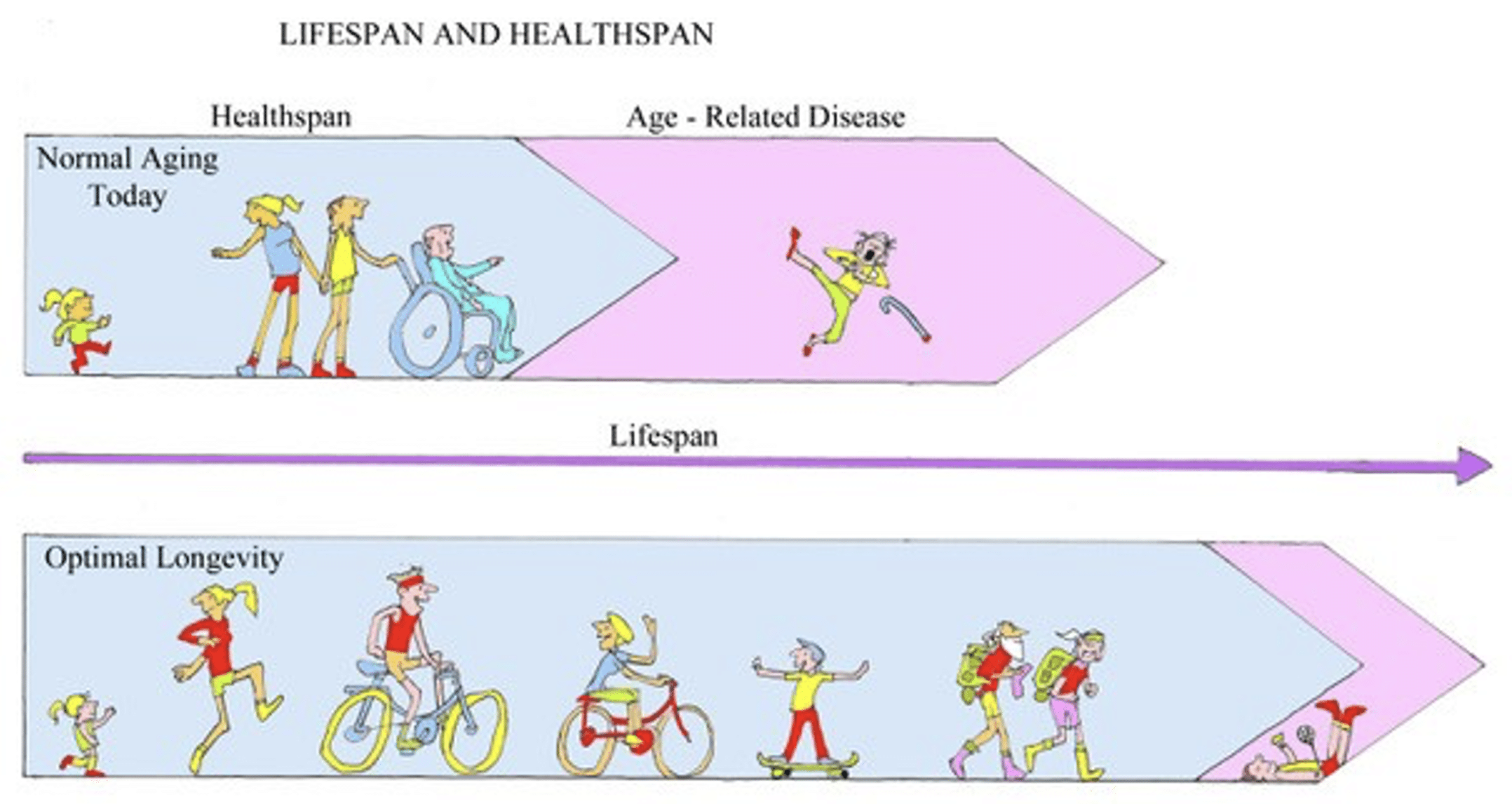
Lifespan and healthspan
Another way of viewing the effects of regular exercise on the ageing process is provided by the notion of ‘healthspan’. We are all familiar with the term ‘lifespan’ indicating total length of life. Healthspan is the length of healthy life and is, I believe, far more important than lifespan. The time between the end of healthy living and end of life is the period of living with one or more disabilities. These include frailty and all the NCDs mentioned above that can limit activity and general enjoyment of life during this period of ‘terminal morbidity’!
The more physically active you are, the longer both your healthspan and lifespan are.10 The increase in healthspan is greater than the increase in lifespan so the period of terminal morbidity is lessened. If Granny exercises regularly, her period of dependence at the end of life is greatly shortened — she lives well and long to the end or near the end of her life.
An active Granny has fewer years of disability at the end of her life than an inactive Granny. The relative increase in healthspan is considerably greater than for lifespan and thus the shorter the period from the end of healthspan to the end of lifespan.
The Department of Health and Social Care recommends that we take 150 minutes per week of moderate-intensity exercise, with strength/balance exercise on 2 days of the week.11 The improved health status of older people who have exercised regularly has been well illustrated by one study, which found that the average 65 year old can expect an additional 12.7 years of healthy life — meaning that he or she will live disability free until aged 77.7. Highly active 65 year olds, however, have an additional 5.7 years of healthy life expectancy — they will remain disability free until aged 83.4 years.
In the ideal scenario, Granny lives well into old age and dies very soon after the onset of dependence.
What are the consequences of frailty?
The main consequences are debility, dependence, and greatly increased risk of acute illness. The frail are very prone to infections, falls, fall-related fractures, and acute exacerbations of pre-existent disease such as heart attacks or strokes. Most of acute hospital admissions are of conditions like these and lead to the cascade of problems that have received so much attention recently. Working backwards, there are insufficient care home places and carers in the community SO people who no longer need hospital treatment languish in the scarce beds SO the accident and emergency department is full of patients for whom no bed can be found SO ambulances queue outside the hospital SO there is no ambulance to attend the old lady who has broken her hip.
So what should Granny do?
“The more physically active you are, the longer both your healthspan and lifespan are.”
In the ideal world, Granny is an active and physically fit person who is as well protected as she can be by her healthy lifestyle. It is important that she maintains this lifestyle despite any limitations put on her by restrictions or lockdowns. Unfortunately, the restrictions imposed on the population in response to the pandemic led to a general decrease in physical activity and contributed to cardiopulmonary deconditioning.12 Already vulnerable older people have been made even more vulnerable.
To reverse this trend, Granny needs more exercise to prepare her to combat any infection. The idea of this ‘prehabilitation’ is not new. It was used soon after World War 2 and nowadays is applied to improve the outcome of major surgery for unfit patients.13 If Granny is inactive and unfit she will also benefit from prehabilitation to improve her ability to fight infection and survive COVID-19 if she is unlucky enough to catch it.
The best protection for Granny in these uncertain times is getting fitter. She can go to the gym, walk more, cycle (three wheelers are ideal), do more in the garden or around the house, or join a Zoom exercise group. These are much better options than condemning her to a lonely death in a care home or incarcerated in her own home, visited only by professional carers.
The greater good
If enough Grannies follow this advice, many more will be able to stay at home and look after themselves. Care homes will not become totally redundant but their resident populations will shrink considerably — to the benefit of Grannies themselves, their own and their families’ finances, and the finances of the country as a whole.
So, don’t kill Granny — save her life by sending her to the gym.
References
1. Xue Q-L. The frailty syndrome: definition and natural history. Clin Geriatr Med 2011; 27(1): 1–15.
2. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci 2001; 56(3): M146–M156.
3. Doherty TJ. Ageing and sarcopenia. J Appl Physiol (1985) 2003; 95(4): 1717–1727.
4. Shephard RJ. Maximal oxygen intake and independence in old age. Br J Sports Med 2009; 43(5): 342–346.
5. Fleg JL, Morrell CH, Bos AG, et al. Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation 2005; 112(5): 674–682.
6. Tidy C, Knott K. Prevention of falls in the elderly. 2022. https://patient.info/doctor/prevention-of-falls-in-the-elderly-pro (accessed 10 Mar 2025).
7. Brennan MM. Movement is muscle in hospitalized adults. Geriatr Nurs 2024; 55: 373–375.
8. Pollock RD, Carter S, Velloso CP, et al. An investigation into the relationship between age and physiological function in highly active older adults. J Physiol 2015; 593(3): 657–680.
9. Chou W-T, Tomata Y, Watanabe T, et al. Relationships between changes in time spent walking since middle age and incident functional disability. Prev Med 2014; 59: 68–72.
10. Office for National Statistics. Health and life expectancies. https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/healthandlifeexpectancies#publications (accessed 10 Mar 2025).
11. Department of Health and Social Care, Office for Health Improvement and Disparities. Physical activity guidelines. 2023. https://www.gov.uk/government/collections/physical-activity-guidelines (accessed 18 Mar 2025).
12. National Institute for Health and Care Excellence (NICE). COVID-19 rapid guideline: managing the long-term effects of COVID-19. London: NICE, 2024. https://www.nice.org.uk/guidance/ng188 (accessed 10 Mar 2025).
13. Durrand J, Singh SJ, Danjoux G, Prehabilitation. Clin Med (Lond) 2019; 19(6): 458–464.
Featured photo by George Pagan III on Unsplash.




