Jim Brockbank has retired from general practice. He continues in his role as a GP appraiser and as an international Royal College of General Practitioners trainer for Myanmar.
Jim Brockbank has retired from general practice. He continues in his role as a GP appraiser and as an international Royal College of General Practitioners trainer for Myanmar.
The hope of democracy and a universal healthcare system by 2030 in Myanmar was brought to an abrupt halt by the military coup of 1 February 2021 and has previously been discussed in the BJGP.1 Five years later, this brutal, largely forgotten civil war continues but so do the efforts to support health professionals including GPs. Violations of medical neutrality continue, not forgetting COVID-19, Cyclone Mocha, and an earthquake during this 5-year period.
From 2021 to 2025, at least 906 health workers have been arrested, 1829 attacks carried out against health workers and infrastructure, and 165 health workers have been killed.2 Medicines are in short supply and expensive due to the deliberate destruction of supply chains, with rising cases of tuberculosis, HIV, and malaria.3
Our medical and nursing colleagues continue to display the best of humanity in providing health care to their communities in such circumstances, they are so deserving of our support.
The Royal College of General Practitioners Quality Improvement project
As discussed previously in this journal, the project commenced in 2018 and continued remotely after COVID-19 and the coup.1,3,4 Nearly 500 Myanmar GPs in 50 townships have completed the introductory Quality Improvement (QI) courses. A course handbook has been developed that is digitally available for all participants, key topics include:
• infection control;
• medical records;
• case review and learning from patients;
• audit;
• quality circles (peer group learning);
• professional development plans (PDPs);
• significant event analysis; and
• consultation skills.
“A strong network of support for colleagues in Myanmar has been developed.”
Examples of sustainability include the development of examples of QI by Myanmar colleagues. Another example is the development of a Teaching of the Teachers (ToT) course in 2024. Royal College of General Practitioners (RCGP) trainers provide mentoring, support, and teaching on topics that include:
• review of QI techniques;
• introduction to adult learning;
• how to give a good PowerPoint presentation;
• how to run a small group;
• proficiency in remote teaching; and
• how to give feedback.
Sixteen Myanmar GP QI trainers will have taught 225 GP colleagues on the QI Introduction course by the summer of 2026.
Diffidence in giving direct negative feedback is a cultural factor we needed to acknowledge. We have emphasised the value of constructive feedback and use established feedback techniques.
Outcomes of the project include improvement in infection control, confidence to develop medical records, peer group learning, and developing PDPs. ToT graduates gain the confidence and skills required to successfully teach QI to colleagues.
Telemedicine
Telemedicine is as an innovative re-imagined primary source of care in Myanmar that promotes shared purpose and resilience. The telemedicine project started after the coup in partnership with Cambridge Global Health Partnerships; 23 000 teleconsultations to 93 000 patients from 322 townships have since taken place. The scope was expanded to include the earthquake emergency relief operation and mental health services for affected communities.
RCGP trainers have contributed to the quality assurance of the telemedicine services; for example, an audit of digital records from primary care clinics using a scoring framework based on NHS standards for record keeping demonstrated more than 80% of the records audited had a record of diagnosis, consultation details, and overall clarity. Documentation compliance was lower for past medical history (PMH) and onward referral details; subsequently, documentation of PMH and referral details became compulsory (Aung S, personal communication, 2024). Myanmar RCGP trainers who have graduated from the ToT course also deliver QI training to Myanmar doctors working in telemedicine. The RCGP will observe this training and provide feedback to the trainers (Aung S, personal communication, 2024).
“… our aspiration to develop a nucleus of Myanmar GPs with QI skills who are able to provide quality care to patients continues.”
Webinars
Between 60 and 80 Myanmar GPs attend monthly webinars that are organised by the RCGP trainers; Myanmar GPs are asked to identify their learning needs. Topics have included common ear, nose, and throat problems, diabetes, care of older persons, management of sepsis, and management of atrial fibrillation. Continuing the monthly webinars reminds Myanmar colleagues they have not been forgotten.
Internally displaced people
Almost one-third of Myanmar’s population (16.2 million) now require urgent humanitarian assistance5 — nearly 4 million have been displaced by conflict and earthquake.6 The junta has deliberately restricted humanitarian aid, preventing essential medicines from reaching ethnic regions and border areas where displaced populations seek refuge. These blockades enable the spread of preventable diseases and routine immunisation programmes have collapsed in many areas.7 This mass displacement has overwhelmed Myanmar’s healthcare system.
Our work has expanded to include ethnic border organisations working with displaced populations, one such organisation is the Mae Tao Clinic on the Thailand–Myanmar border. RCGP trainers have made six monthly visits to the clinic since November 2023 that comprise 5-day interactive workshops on QI activities for healthcare staff. Attendees include doctors, clinical managers, nurses, and nurse aids, totalling 25–30 participants. Monthly seminars online are undertaken between the clinic visits. Outcomes include:
• diabetes and drug chart audits completed;
• monthly QI team meetings led by a QI manager;
• staff development of individual PDPs;
• significant event analyses regularly discussed; and
• individual and organisational learning undertaken.
Health partnerships for Myanmar
Convened by Global Health Partnerships, formerly the Tropical Health and Education Trust, representatives from over 30 institutions, including the medical Royal Colleges, have met online monthly since the coup to support colleagues delivering health care. A strong network of support for colleagues in Myanmar has been developed.
COVID-19 and an earthquake
It’s hard to understand the actions of a leadership that attacks doctors and nurses at the peak of a pandemic, but that is what happened in Myanmar. Medics feared arrest or detention at a time when Myanmar needed them most.4
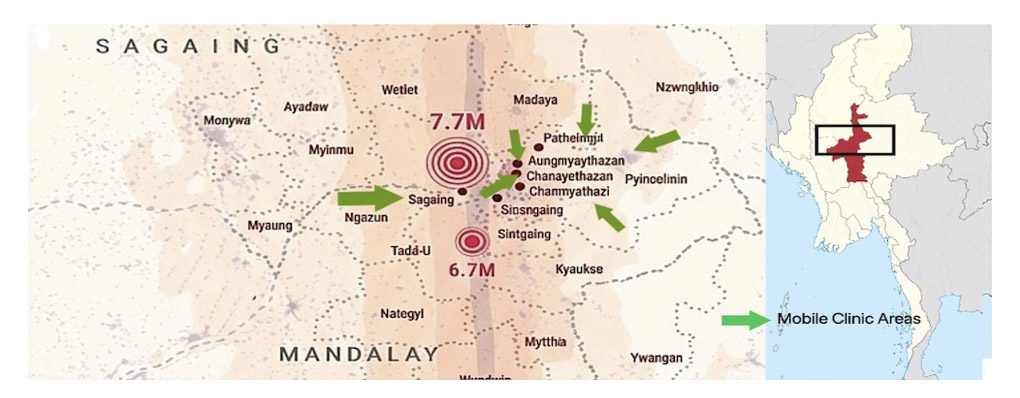
Following the earthquake in March 2025, when rescuers were digging through rubble with their bare hands and bodies piled up in mass graves, the junta gave the command to recommence bombing. The military also obstructed relief efforts in resistance-held areas, just as they had done during Cyclone Mocha in 2023. In contrast, GPs deployed mobile clinics within 72 hours, treating survivors in temporary shelters (Aung S, personal communication, 2025).

What have we learnt and what next?
In times of conflict, the need to update knowledge and strengthen skills as clinicians could so easily not be a priority, but our colleagues in Myanmar have embraced the expansion of a sustainable programme of QI training and continuing medical education. One of the key outcomes has been the promotion of collaborative learning through expansion and networking of quality circles across Myanmar.
The internet allows us to reach colleagues in remote and conflict-ridden locations but we need to be alert to security risks.
Partnerships matter and provide a rich source of support, collaboration, advocacy, and education. It is a remarkable achievement that Health Partnerships for Myanmar (HPfM) has continued to meet over a 5-year period since the coup. Connections across partnerships are made and it is through HPfM that RCGP trainers have worked collaboratively with the telemedicine project in Myanmar.
We can’t know what the future holds for Myanmar and its people but our aspiration to develop a nucleus of Myanmar GPs with QI skills who are able to provide quality care to patients continues.
References
1. Brockbank J. The dream of universal healthcare in Myanmar becomes a nightmare. BJGP Life 2021; 29 Mar:
https://bjgplife.com/2021/03/29/the-dream-of-universal-healthcare-in-myanmar-becomes-a-nightmare (accessed 25 Mar 2026).
2. Insecurity Insight. Attacks on health care in Myanmar. 2026. https://insecurityinsight.org/wp-content/uploads/2026/01/83.-24-December-2025-06-January-2026-Attacks-on-Health-Care-in-Myanmar-.pdf (accessed 25 Mar 2026).
3. Brockbank J. GP education amid the conflict in Myanmar. BJGP Life 2024; 5 Feb: https://bjgplife.com/gp-education-amid-the-conflict-in-myanmar (accessed 25 Mar 2026).
4. Brockbank J. The chaos of Covid in Myanmar. BJGP Life 2021; 22 Sep: https://bjgplife.com/the-chaos-of-covid-in-myanmar (accessed 31 Mar 2026).
5. United Nations Office for the Coordination of Humanitarian Affairs. Asia and the Pacific: Myanmar. 2026. https://www.unocha.org/myanmar (accessed 31 Mar 2026).
6. United Nations High Commissioner for Refugees. Estimated Myanmar refugees and asylum seekers. 2026. https://data.unhcr.org/en/situations/myanmar (accessed 31 Mar 2026).
7. Wooton M, Foster J, Lwin MM, et al. Caring for children in conflict: virtual nursing resources during the 2021 Myanmar coup and ensuing civil war. Nurs Child Young People 2026; DOI: 10.7748/ncyp.2026.e1576.
Featured photo provided by a Myanmar colleague and used with permission. Damage caused by earthquakes in March 2025.