

 Nic Dickson is a researcher, visual artist, and adult educator who creates hand-drawn and digital images to capture and disseminate research. Her visual note projects can be found at https://visualinquiry.co.uk.
Nic Dickson is a researcher, visual artist, and adult educator who creates hand-drawn and digital images to capture and disseminate research. Her visual note projects can be found at https://visualinquiry.co.uk.
Leanne McBride is a dedicated community activist and facilitator for Chance 2 Change, a peer support group in Drumchapel focused on amplifying community voice to address health inequalities.
Colette Mason is a Community Links Worker Programme Manager with the ALLIANCE in Glasgow and West Dunbartonshire, she sits on the GPs at the Deep End steering group. She is on X: @letsmakeslinks
Fraser Devine is Lead Operations Manager at Men Matters Scotland, a charity that exists to prevent suicide and promote positive mental wellbeing in men.
Marianne McCallum is an academic GP, working in both Clydebank and Glasgow University, and a steering group member of GPs at the Deep End. She is on Bluesky: @mars-mcc.bsky.social
‘Health systems are typically designed by healthy people, and we typically design them in our own image.’ — Adam Burley, Clinical Psychologist Trauma and Exclusion Health, speaking at the Deep End conference, 12 April 2024.
Community shapes health
The communities we live in, and our life encounters, influence our decisions and actions. Failing to consider the diverse experiences of those facing socioeconomic disadvantage or marginalisation leads to services that align with central policy but may not meet the needs of our communities.
GPs at the Deep End is a network of regional groups of primary care practitioners working in areas of high socioeconomic deprivation, known as the ‘Deep End’. They use advocacy, research, training, and peer support to explore how primary care can reduce inequalities.1 At their recent international conference, we led a workshop on meaningful community engagement in a Deep End context.
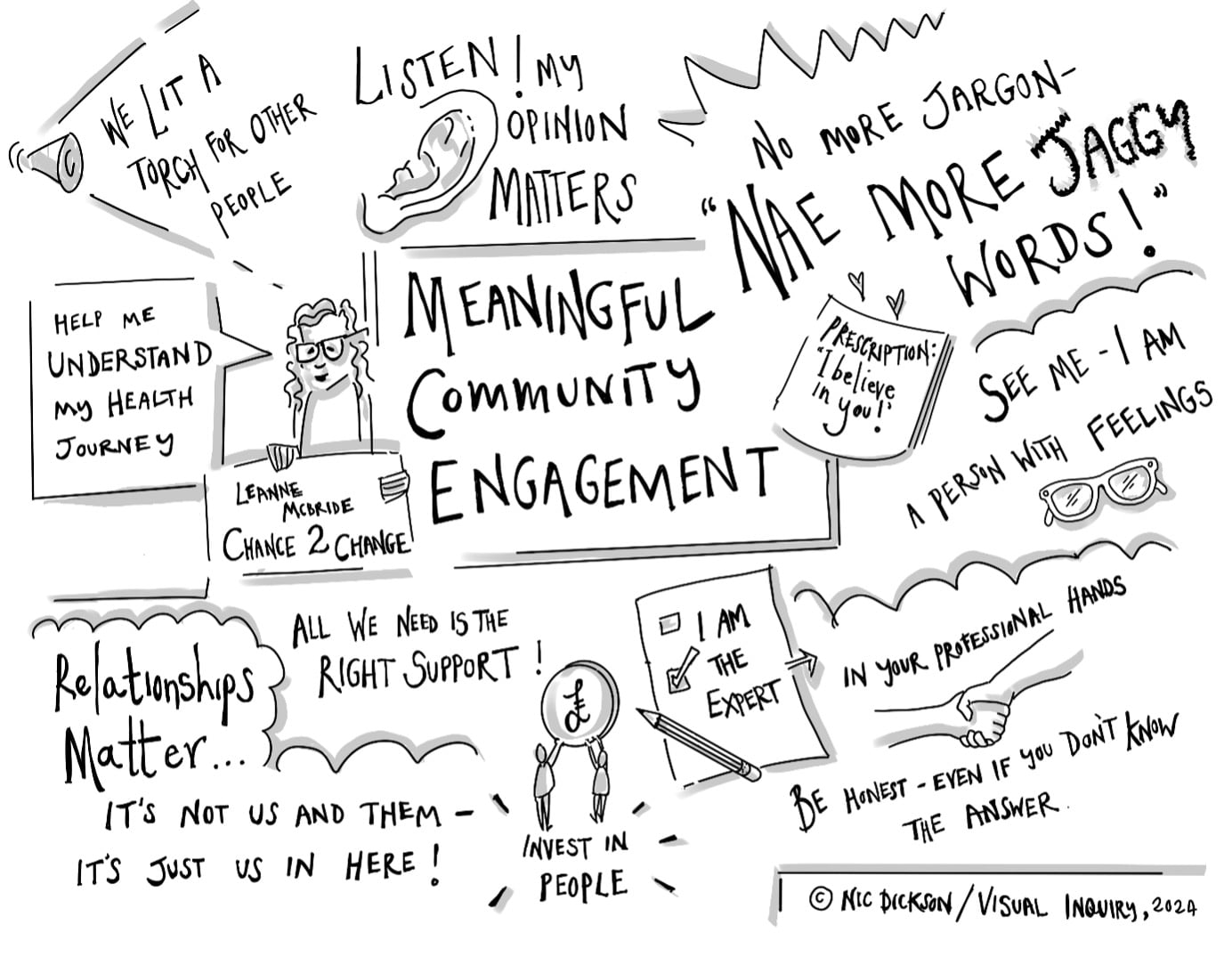
“… take time to listen and understand, stop using ‘jaggy words’ (jargon), and embrace partnership working and our patient’s expertise.”
The importance of tailoring services to different communities was illustrated during the conference ceilidh (traditional Scottish dance). While natives twirled through dances they had been taught in primary school, others gamely followed instructions from the band or were just confused.
It may be a simple example, but IF the next UK flagship exercise strategy was weekly ceilidhs in all communities, clear issues of fairness/disadvantage would emerge. It preferentially benefits one group; those who know, and have been doing, the dances since childhood. It COULD work for others if a teaching budget was included. If not, some may still try but will likely not get the full benefit.
This hypothetical example illustrates how not considering the community context may favour or discriminate different populations. Whether community factors may limit application of clinical guideline is rarely considered. Additional resources that may be required to do so are seldom provided or acknowledged. Instead, people are blamed for ‘not engaging’.
Community-based solutions
The workshop heard about peer mentors from Chance 2 Change and Men Matter Scotland. Peer support can be transformative; there is strength and resilience in many of our Deep End communities. We may not have material wealth, but we are rich in community spirit. Through peer support, communities can create authentic solutions to promoting wellbeing in ways professionals cannot.
Practitioners who understand a community (good and bad) are essential. High-quality relational continuity of care can support change in even the most challenging of circumstances.2 Leanne McBride powerfully shared the difference her own GP’s ‘I believe in you’ prescription made in tough times. We captured her talk as a visual note (Figure 1), which gave advice to GPs from Chance 2 Change. McBride called on us (professionals) to take time to listen and understand, stop using ‘jaggy words’ (jargon), and embrace partnership working and our patient’s expertise.
Linking community and primary care
Many practices may see the value of collaborating with ongoing community efforts. However, practitioners are under significant pressure, leaving little opportunity for community engagement, even if many may want to. This is especially pronounced for Deep End practices, where the disparity between available resources and community needs is particularly stark.3
“The Deep End project demonstrates change can be made by practitioners working together to advocate for primary care to be at its best where it is needed most.”
Community links workers (CLWs) can act as bridges between practices and communities. In Glasgow Deep End practices the CLWs, employed by the third-sector Health and Social Care Alliance, have protected time to build community connections. Releasing the potential of the CLW may require recognition and protection of the community aspects of the role in the face of increasing demand.
There are no easy answers: workshop attendees acknowledged the current ‘epidemic of exhaustion’ within the third sector and the NHS, with funding precarity a particular issue for the third sector. Peer support cannot be a cheap alternative to services. It requires supportive integration to ensure it is sustainable and not exploitative.
Where do we go from here?
Coalface practitioners know relational continuity of care and awareness of community dynamics enhance our effectiveness. While more difficult to measure than an HbA1c, they are also markers of quality of care. Advocating for resources supporting relational continuity of care and developing guidelines and interventions tailored to, rather than imposed on, communities is essential.
The Deep End project demonstrates change can be made by practitioners working together to advocate for primary care to be at its best where it is needed most. As a professional group, we hold more power than we realise. If we do not advocate for relational continuity of care, supported by a deep understanding of the communities we serve, then who will?
References
1. Scottish Government Primary Care Directorate. Primary Care Health Inequalities Short-Life Working Group recommendations: progress report 2023. 2023. https://www.gov.scot/publications/progress-report-2022-recommendations-primary-care-health-inequalities-short-life-working-group (accessed 31 Jan 2025).
2. McCallum M, MacDonald S, Mair FS. Multimorbidity and person-centred care in a socioeconomically deprived community: a qualitative study. Br J Gen Pract 2024; DOI: https://doi.org/10.3399/BJGP.2024.0286.
3. Fisher R, Dunn P, Asaria M, Thorlby R. Briefing: Level or not? Comparing general practice in areas of high and low socioeconomic deprivation in England. 2020. https://www.health.org.uk/sites/default/files/upload/publications/2020/LevelOrNot_Web1_0.pdf (accessed 31 Jan 2025).
Featured photo by Jonathan Borba on Unsplash.





[…] (Community Links Worker manager) and Frazer Devine (Men Matter Scotland). It has been published in BJGP Life and will appear in the British Journal for General Practitioners on 28th March 2024. The opinion […]