

Padmini Parthasarathi is a GP ST3 under St Georges Vocational Training Scheme.
Morag M Lenman is a GP at Nightingale Practice.
The COVID-19 pandemic of 2020–2021 has drastically changed the face of the world. Every country has been affected and sadly there has been considerable loss of life. Unlike the Spanish flu pandemic of 1918, where large numbers of young people died, COVID-19 is a virus that causes mortality predominantly in the elderly and frail population. Therefore, it is no surprise that losses have been particularly heavy in the care home sector.1
As always, the strength of the human spirit has shone through the darkness. There have been incredible success stories, such as that of the vaccination programme, implemented with incredible speed and on an unprecedented scale. Our care home, Nightingale House in South-West London, has been through a rollercoaster journey over the course of the pandemic and we would like to tell our story.
Nightingale is unusual for a care home, given its large size (200 beds) and the fact that all residents are Jewish, with an average age of over 90 years. It was clear from the outset of the pandemic that it was going to have a profound impact on our residents. Furthermore, as most of our residents are severely frail and not appropriate for escalation to hospital, we knew we had to face the battle with COVID-19 within the care home setting.
Some commentators in 2020 questioned why care home residents were being prioritised for vaccination when their life expectancy was low. We will illustrate the devastating impact of COVID-19 on this patient population, the reason for prioritisation, and why vaccination was a lifeline for this group.
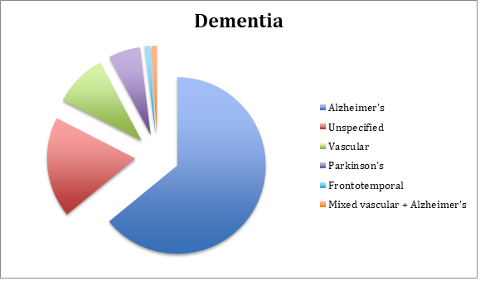
We have looked at patient records in the calendar year 2020, which encompassed two ‘waves’ of COVID-19 and the much-awaited introduction of the vaccination programme. Here is a demographic snapshot of the residents at the start of 2020:
| Age of resident, years | |
| Mean | 88 |
| Mode | 95 |
| Median | 90 |
| Youngest | 58 |
| Eldest | 108 |
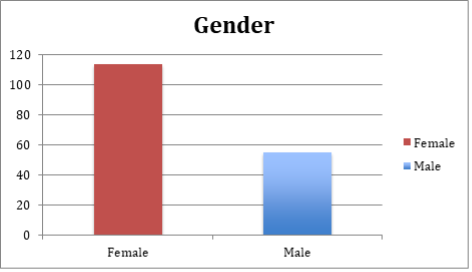
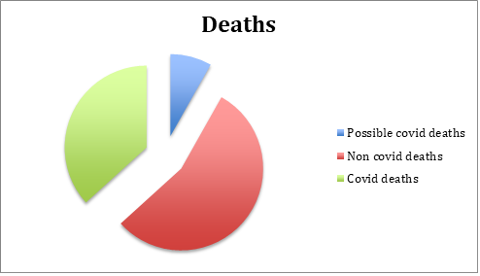
The total number of residents in the care home was 169 at the start of 2020 and fell to 117 by the end of the year. This drastic fall in numbers was due to 3 leavers and 49 deaths. Of the 49 patients who died, 18 of these deaths were attributable to COVID-19 on their death certificates (11 men, 7 women). It is worth noting that among the remaining 31 deaths, a further 4 had symptoms in the 2 weeks preceding their death.
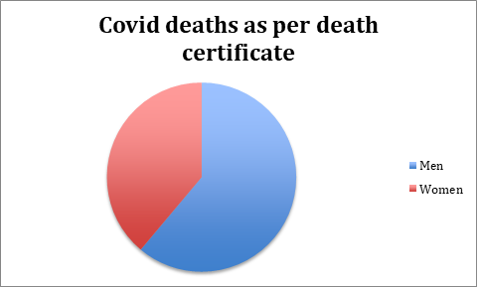
Looking at the official COVID-19 deaths, the average age was 88.7 years. Among the men this average was 87.5 years while the average age of women who died was 90.6 years. The chart above shows that men were far more adversely affected than women.
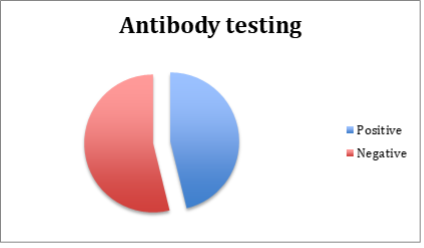
If we analyse this a little further, of the 129 residents who had a COVID-19 test recorded in 2020, 5 tested positive in their first test and 20 of those with an initial negative test actually had COVID-19 symptoms earlier in the year. At that point the UK Government hadn’t implemented nor had the resources for mass testing. A further way to note the impact of COVID-19 in the early part of 2020 before testing was available is to look at serum antibody results. By the end of 2020, of the 65 residents who had had an antibody test, 30 were positive for COVID-19 antibodies.
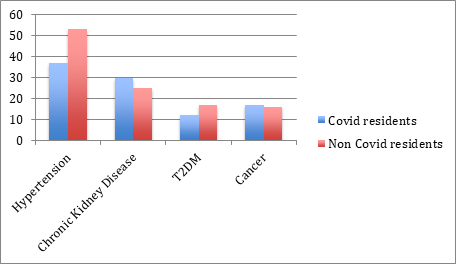
Finally, we looked into the comorbidities of the patients and the relation of this to their COVID-19 status. From various articles and research carried out through the pandemic a few comorbidities were noted to be either more prevalent in COVID-19 patients or cause a more severe infection.2,3 Among our residents there were 80 patients with hypertension, 45 patients with chronic kidney disease, 25 patients with type 2 diabetes, and 27 patients with any type of cancer (excluding skin cancers). Below are the proportions of residents with the specific comorbidity in COVID-19 versus non-COVID-19 patients. We have defined a COVID-19 patient to be anyone with an initial positive COVID-19 test, a positive COVID-19 antibody test, or COVID-19 symptoms in 2020.
Conclusions
COVID-19 had a huge impact on care home residents nationwide. However, there are some other interesting points that come from analysing the above data:
1) While multiple factors have been implicated as possible risk factors for COVID-19 and severity of disease, the biggest risk factor seems to be their age. Comorbidities do not seem to play as big a role as compared to the general population.4
2) As seen in the wider population, men seemed to be affected by COVID-19 more than women, with a higher mortality rate and death occurring at a younger age.5
3) While a huge proportion of our older frail residents did develop COVID-19, most of them actually survived. These patients were managed with supportive care (regular oral fluids and paracetamol), showing that recovery is often possible without hospitalisation and ventilation even in the most vulnerable.
4) The case for vaccination in this cohort is strong. Looking at deaths in 2021 so far, a further 15 deaths have occurred, of which only 3 were attributable to COVID-19. The big difference between 2020 and 2021 is of course the vaccinations that were given at the end of 2020. We had a vaccination uptake of 91% in our residents. Of course, the year is yet to finish, but all the indications are that the vaccination programme was highly protective for our residents and that the huge death toll of 2020 will not be repeated.
The road ahead…
As the year unfolds with new variants, easing of lockdown, and the prospect of a booster vaccination programme, it is uncertain what the future holds. We hope that in sharing Nightingale’s journey through the pandemic in 2020, we have helped you understand how we coped and ultimately protected our residents.
References
1. Alzheimer’s Society. Worst hit: dementia during coronavirus. 2020. https://www.alzheimers.org.uk/sites/default/files/2020-09/Worst-hit-Dementia-during-coronavirus-report.pdf (accessed 25 Aug 2021).
2. Banerjee A, Pasea L, Harris S, et al. Estimating excess 1-year mortality associated with the COVID-19 pandemic according to underlying conditions and age: a population-based cohort study. Lancet 2020; 395(10238): 1715–1725.
3. Honardoost M, Jahani L, Aghili R, et al. The association between presence of comorbidities and COVID-19 severity: a systemic review and meta-analysis. Cerebrovas Dis 2021; 50(2): 132-140.
4. Mueller AL, McNamara MS, Sinclair DA. Why does COVID-19 disproportionately affect older people? Aging 2020; 12(10): 9959-9981.
5. Peckham H, de Gruijter NM, Raine C, et al. Male sex identified by global COVID-19 meta-analysis as a risk factor for death and ITU admission. Nat Commun 2020; 11(1): 6317.
Featured photo by eberhard ✋ grossgasteiger on Unsplash




